



Bladder & urothelial tract
Urothelial carcinoma - invasive
With squamous differentiation
Authors: Chunlai Zuo, M.D., M.S., Huihui Ye, M.D., M.S.
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.

Last author update: 7 May 2024
Last staff update: 7 May 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Urothelial carcinoma with squamous differentiation

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Zuo C, Ye H. With squamous differentiation. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bladdersquamousdiff.html. Accessed July 21st, 2024.
Definition / general
- Urothelial carcinoma with variable amounts of squamous differentiation (intracellular keratin, intercellular bridges or keratin pearls)
Essential features
- Squamous differentiation is the most frequent line of divergent histology seen in high grade urothelial carcinoma (HGUC)
- Approximate percentage of the squamous component should be noted in the report
- Not human papillomavirus (HPV) associated
- Squamous differentiation may be seen in the context of chronic irritation such as with stones, Schistosoma infection and neurogenic bladder with indwelling catheters (Front Med (Lausanne) 2018;5:223, World J Urol 2021;39:1531)
Terminology
- Urothelial carcinoma with squamous differentiation
ICD coding
- ICD-O: 8120/3 - urothelial carcinoma with squamous differentiation
- ICD-10
Epidemiology
- Occurs in 30 - 40% of urothelial carcinomas of bladder (J Clin Pathol 2007;60:332, Urology 2007;70:69)
Sites
- Genitourinary tract (renal pelvis, ureter, bladder and urethra)
Etiology
- Smoking: smoking may increase the risk due to harmful chemicals accumulating in the urine (BJU Int 2008;101:11)
- Aging: urothelial carcinoma can occur at any age; however, most patients diagnosed with urothelial carcinoma are older than 55
- Male gender: men are more likely to develop bladder cancer than women
- Chemical exposure: including arsenic and chemicals used in the manufacture of dyes, rubber, leather, textiles and paint products (Lab Invest 2008;88:686)
- Previous cancer treatment: anticancer drug cyclophosphamide and pelvic radiation treatment (Eur Urol 2019;75:319)
- Longstanding bladder irritation: chronic or repeated urinary infections or inflammations (cystitis), long term use of a urinary catheter (World J Urol 2021;39:1531)
- Family history of cancer: Lynch syndrome with mismatch repair gene mutations (Eur Urol 2013;63:379)
- Neurogenic bladder and HPV infection (Mod Pathol 2012;25:1534)
Clinical features
- Hematuria, dysuria and frequent urination (Urology 2006;67:3)
Diagnosis
- Imaging studies including plain radiograph, ultrasound, computed tomography (CT), magnetic resonance imaging (MRI) (Urol Clin North Am 2018;45:389)
- Cystoscopy
- Biopsy (ultrasound guided biopsy)
- Transurethral resection of bladder tumor (TURBT) (Urology 2006;67:3, Eur Urol Focus 2022;8:457)
- Urine cytology and surgical pathology (Cytopathology 2024;35:199, Urology 2006;67:3)
Laboratory
- Hematuria (red blood cells are identified in urine) is most common
Radiology description
- Contrast filling defect (Cancers (Basel) 2023;15:5040, Urol Clin North Am 2018;45:389)
- Calyces showing distortion / obliteration / amputation (Cancers (Basel) 2023;15:5040)
- Other findings: hydronephrosis or nonfunctioning kidney (Cancers (Basel) 2023;15:5040, Radiographics 2010;30:1553)
Radiology images
Images hosted on other servers:

T1 precontrast demonstrates isoechoic mass

Ultrasound shows mass-like hyperechoic area
Prognostic factors
- Invasive urothelial carcinoma with divergent differentiation has poor prognosis because of common presentation at high stage
- Uncommonly noninvasive urothelial carcinoma showing divergent patterns may not have worse prognosis by limited data
- Stage by stage, no significant association with worse cancer specific survival in comparison with conventional urothelial carcinoma (Urology 2007;70:69, J Urol 2012;188:405)
Case reports
- 62 year old man with differentiation of urothelial carcinoma into 2 distinct subtypes, glandular and squamous, in 3 different organs (Cureus 2020;12:e7280)
- 69 year old White woman with invasive urothelial carcinoma with squamous differentiation and associated high risk HPV infection (Ann Diagn Pathol 2023;63:152103)
- 72 year old man with a primary sarcomatoid urothelial carcinoma of the ureter with heterologous chondrosarcoma and osteosarcoma elements and concurrent divergent squamous differentiation (Urol Case Rep 2020;34:101484)
Treatment
- Surgery: transurethral resection of bladder tumor (TURBT), cystectomy, nephroureterectomy (Ann Diagn Pathol 2007;11:395)
- Chemotherapy (Clin Genitourin Cancer 2024;22:e53)
- Immunotherapy (J Urol 2018;199:1129)
- Radiation therapy (Eur Urol 2017;72:54)
- Targeted therapy (Clin Genitourin Cancer 2023;21:e394)
Gross description
- Lesion may be polypoid, sessile, fungating ulcerated or infiltrative
Gross images
Contributed by Huihui Ye, M.D., M.S.
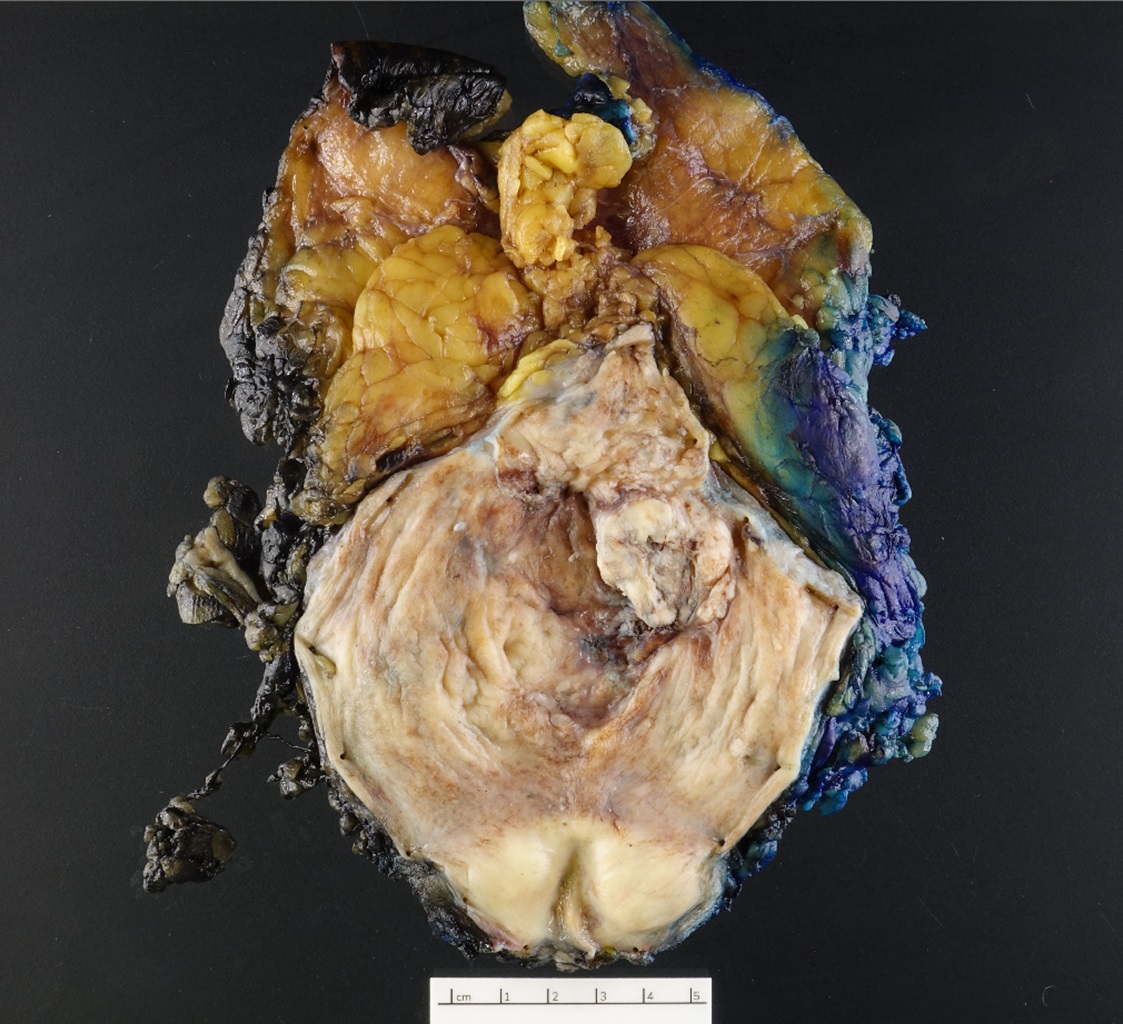
Dome tumor
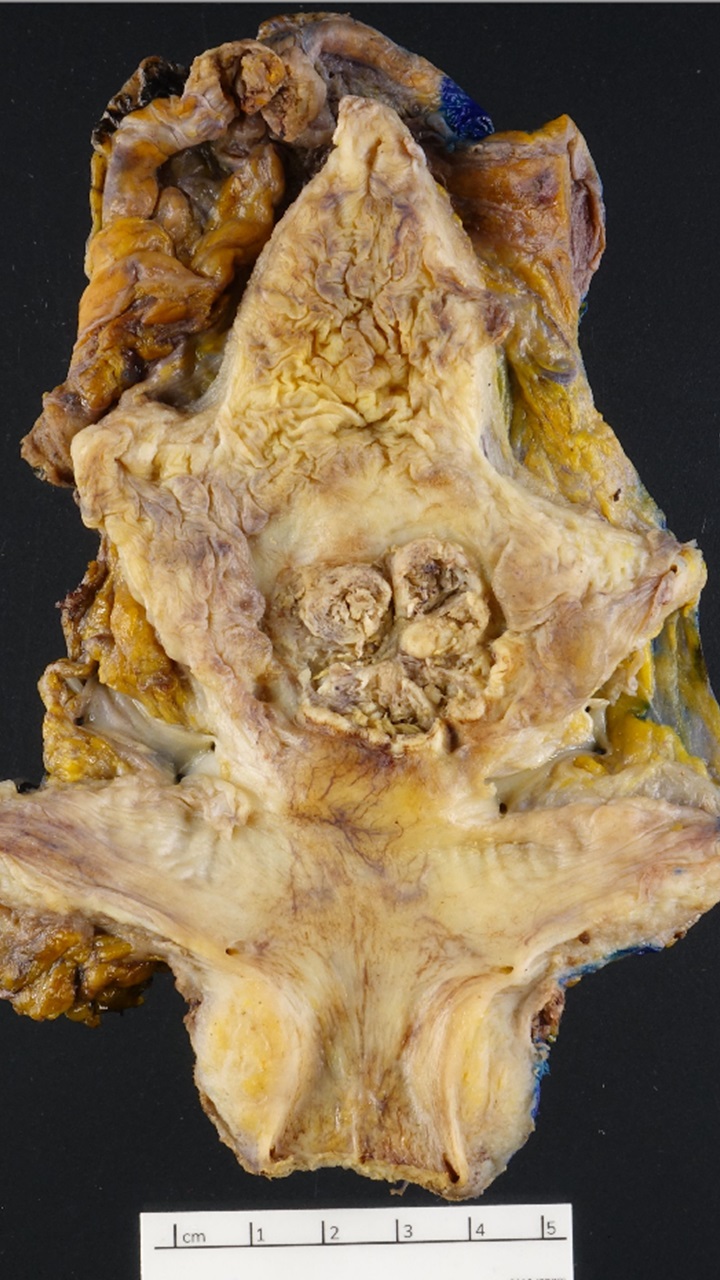
Posterior wall tumor
Microscopic (histologic) description
- Most commonly associated with high grade urothelial carcinoma
- By definition, must have clear cut evidence of urothelial component (invasive urothelial carcinoma)
- Squamous components are similar to typical squamous cell carcinoma: nests of squamous epithelial cells, characterized by large nuclei with abundant eosinophilic cytoplasm and evidence of keratinization (intracellular keratin, intercellular bridges or keratin pearls)
- Squamous component may show basaloid or clear cell features
- Tumor associated eosinophilia in the bladder may present (J Clin Pathol 1984;37:500)
- Presence of squamous component should be reported and providing estimation of the percentage of differentiation is strongly recommended
Microscopic (histologic) images
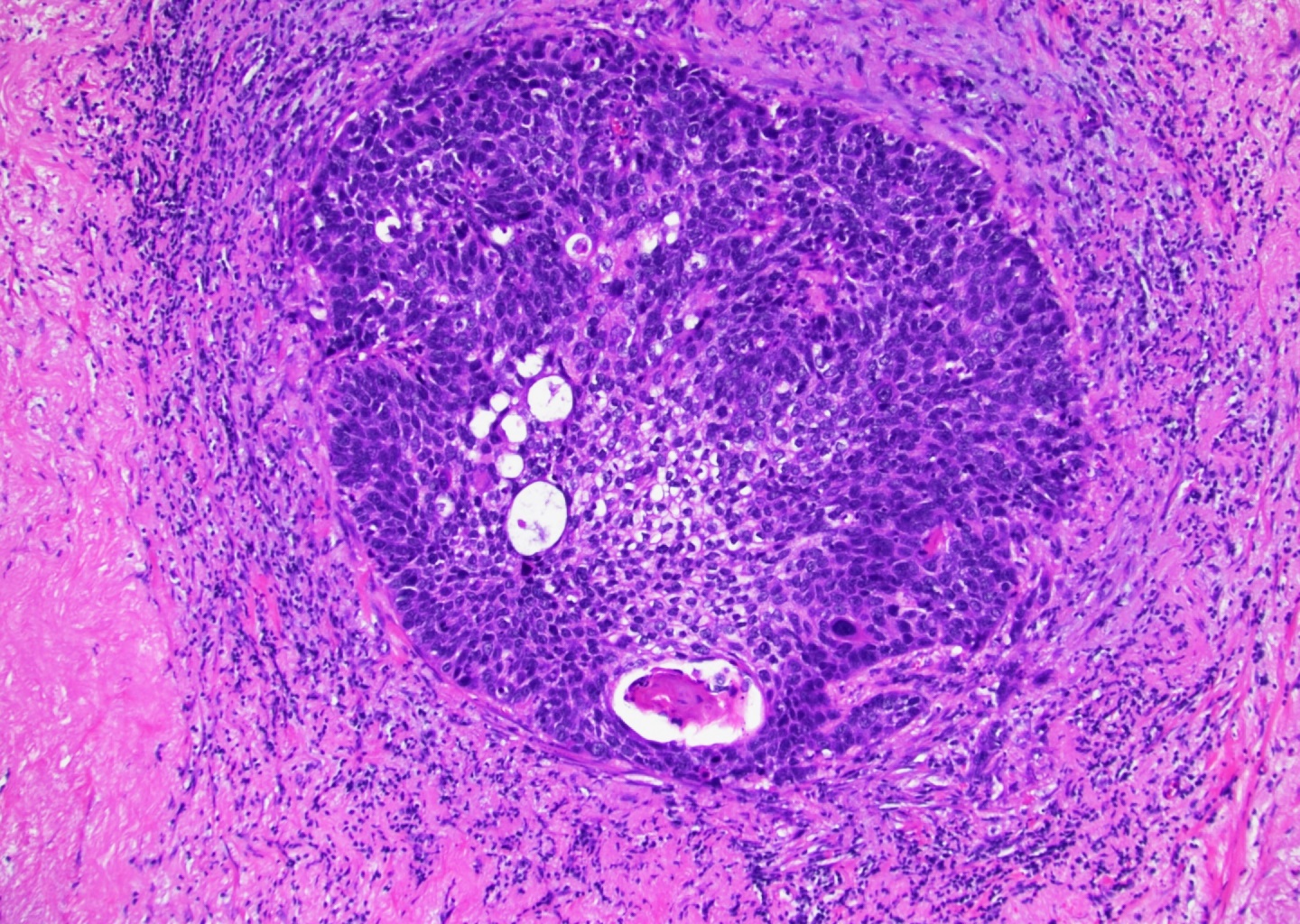
Contributed by Huihui Ye, M.D., M.S.
Basaloid features
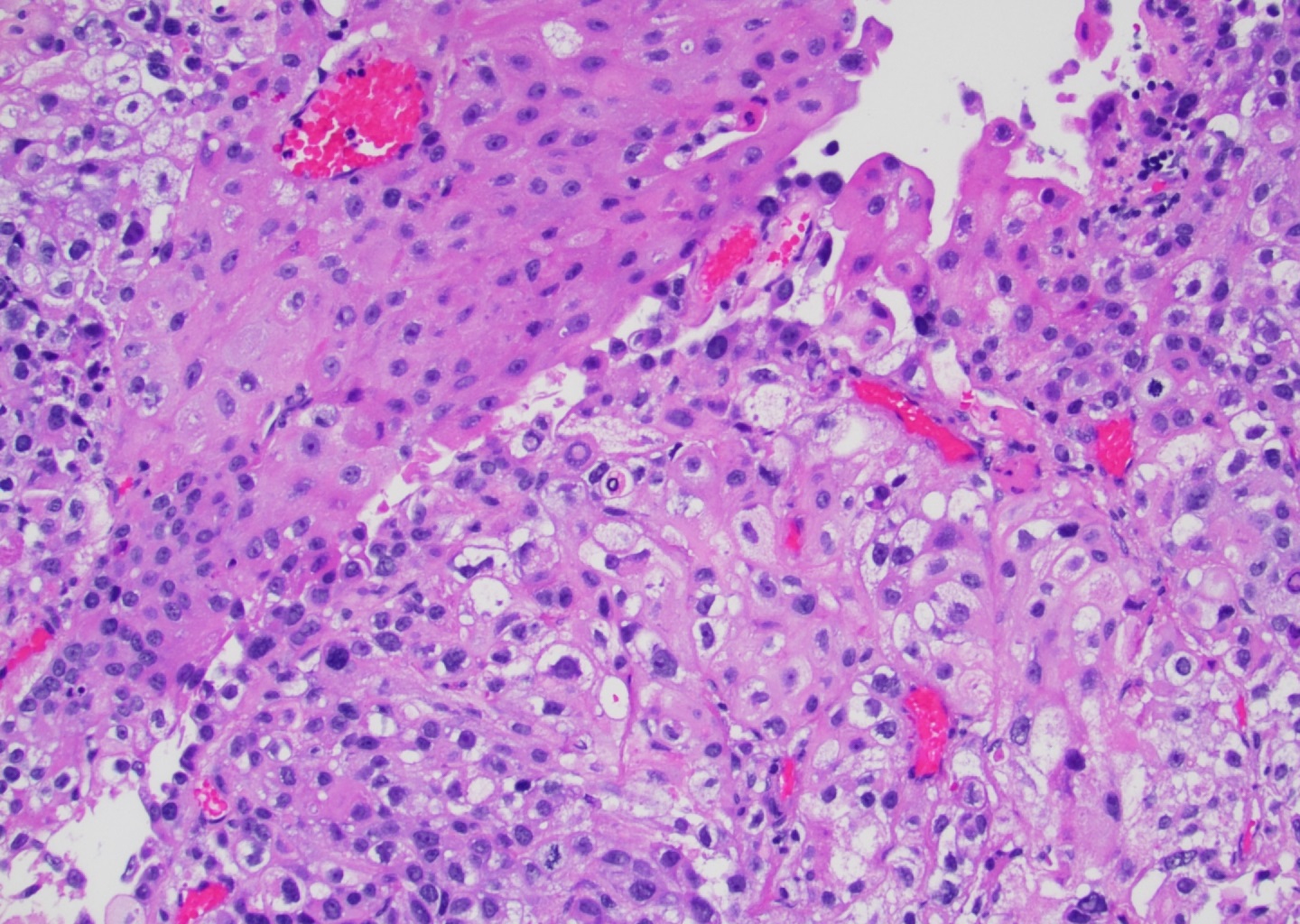
Clear cell features
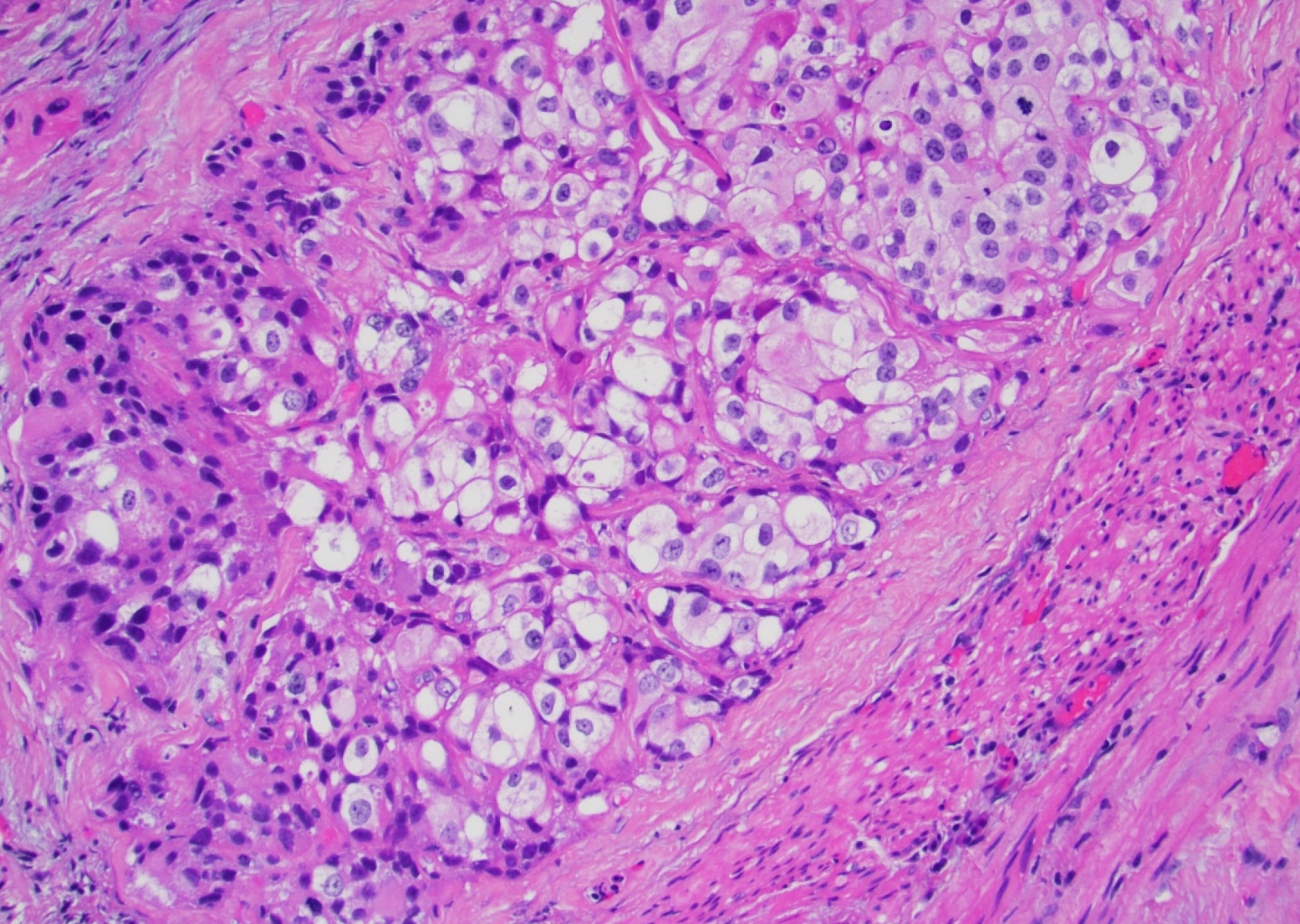
Nests of clear cells
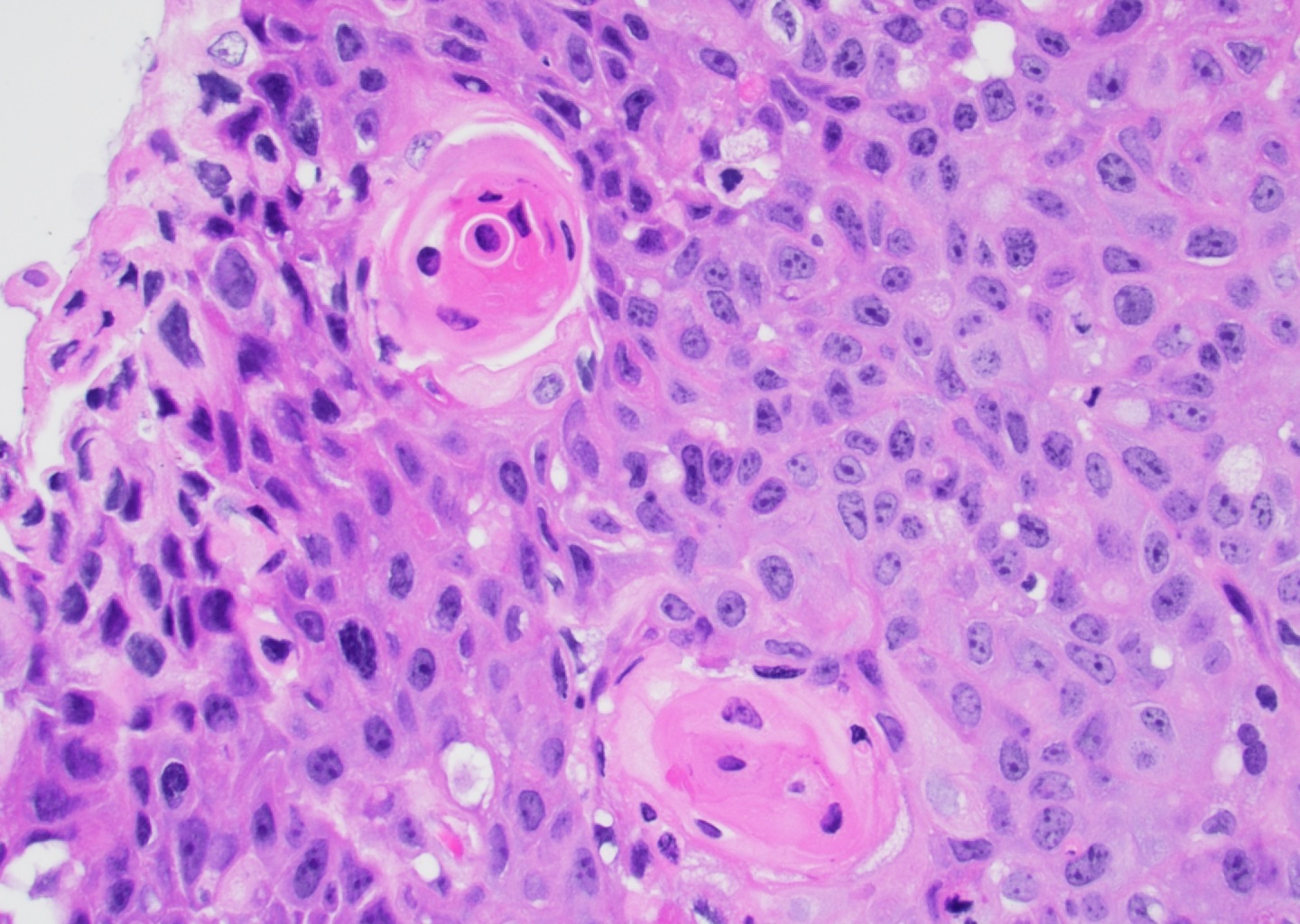
Keratin pearls
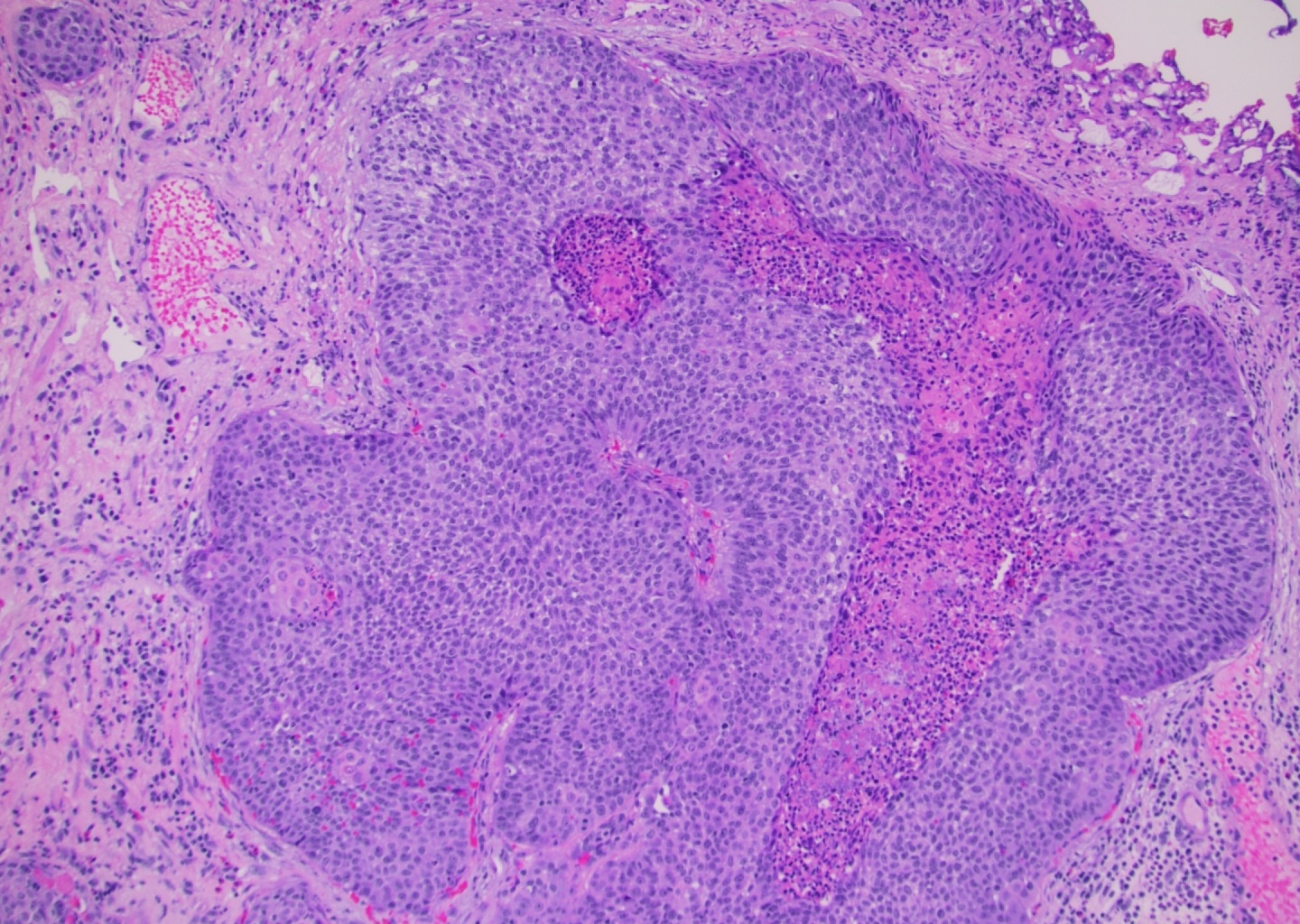
Basaloid with central necrosis
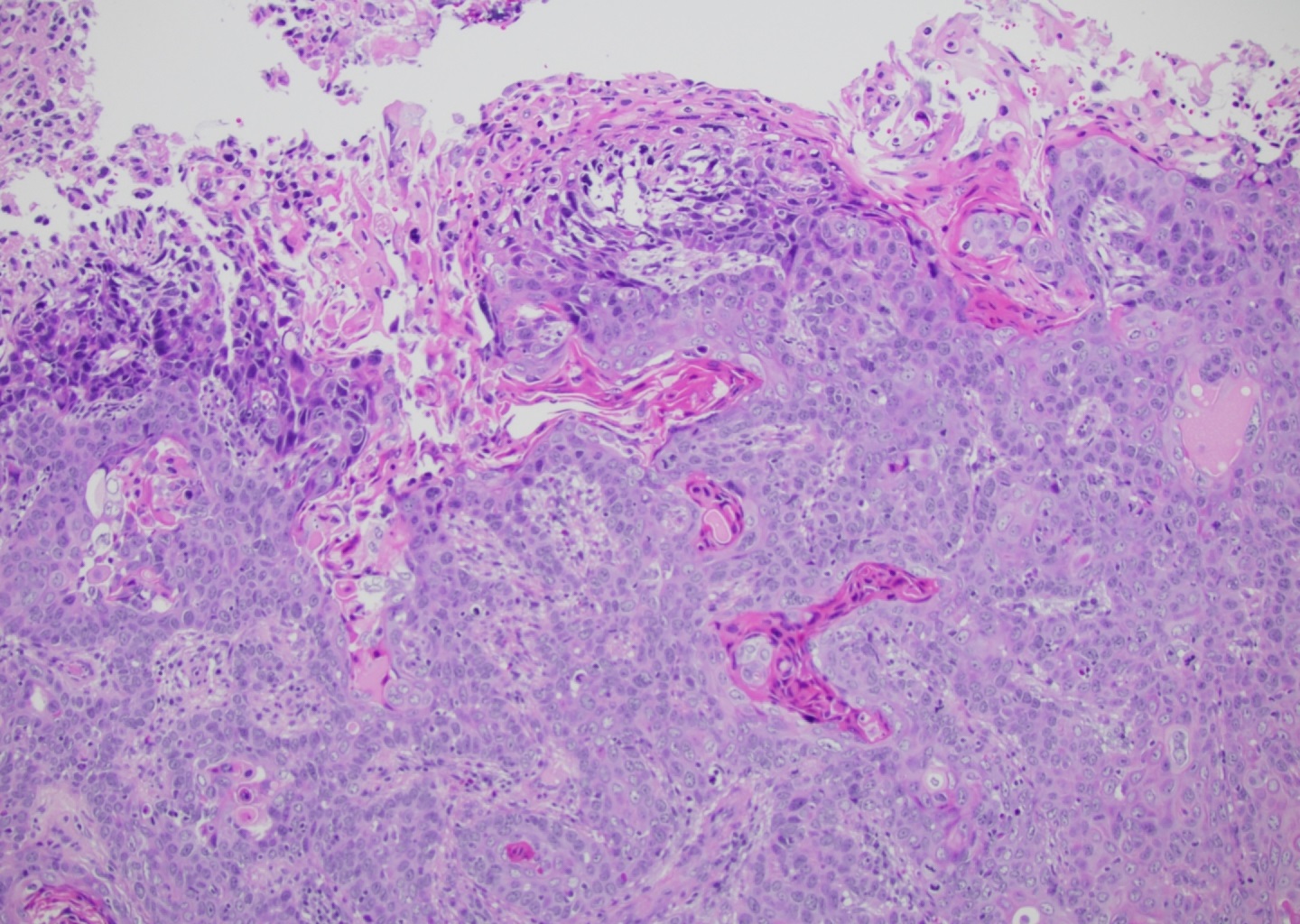
Surface keratinization
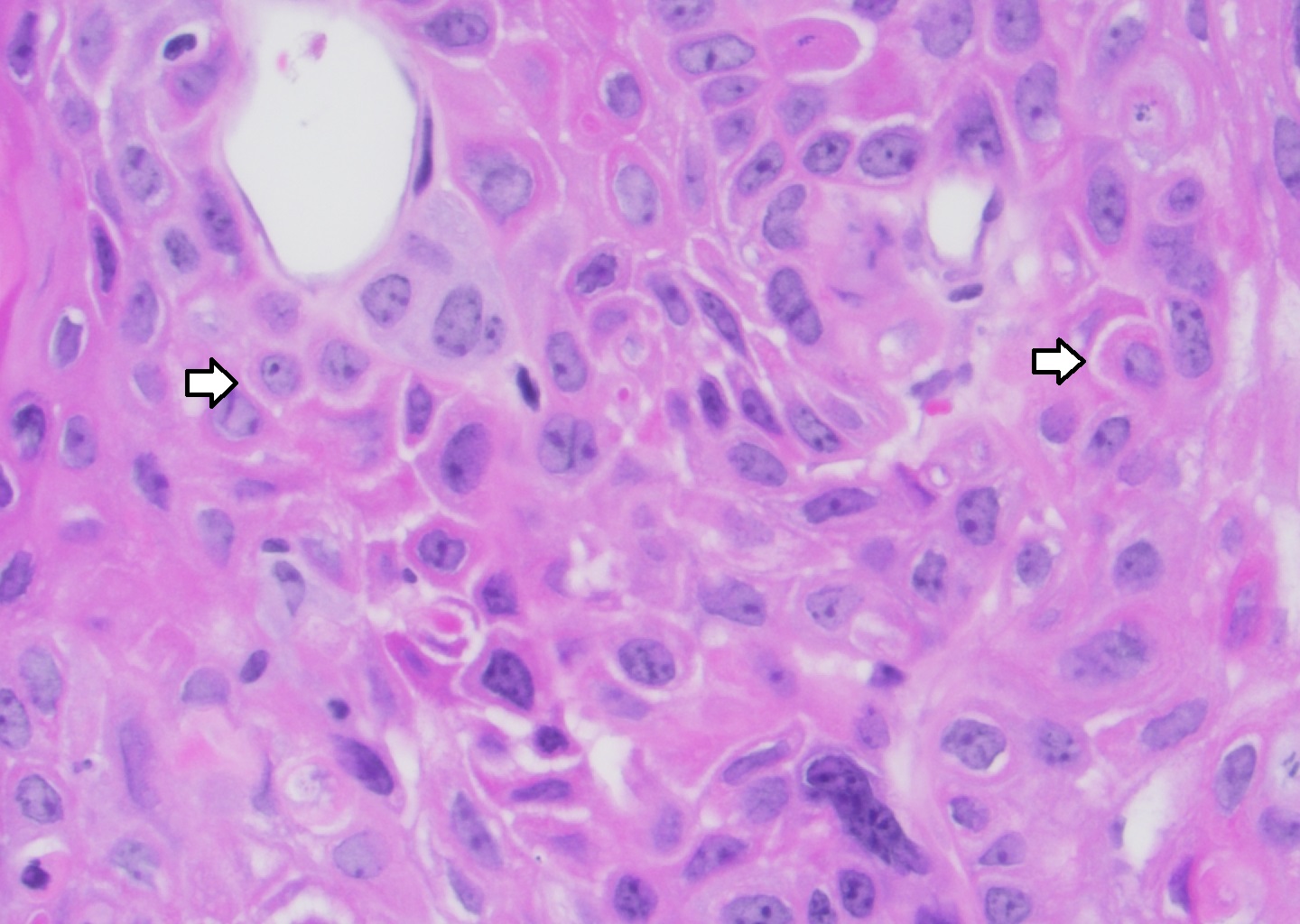
Intercellular bridges
Cytology description
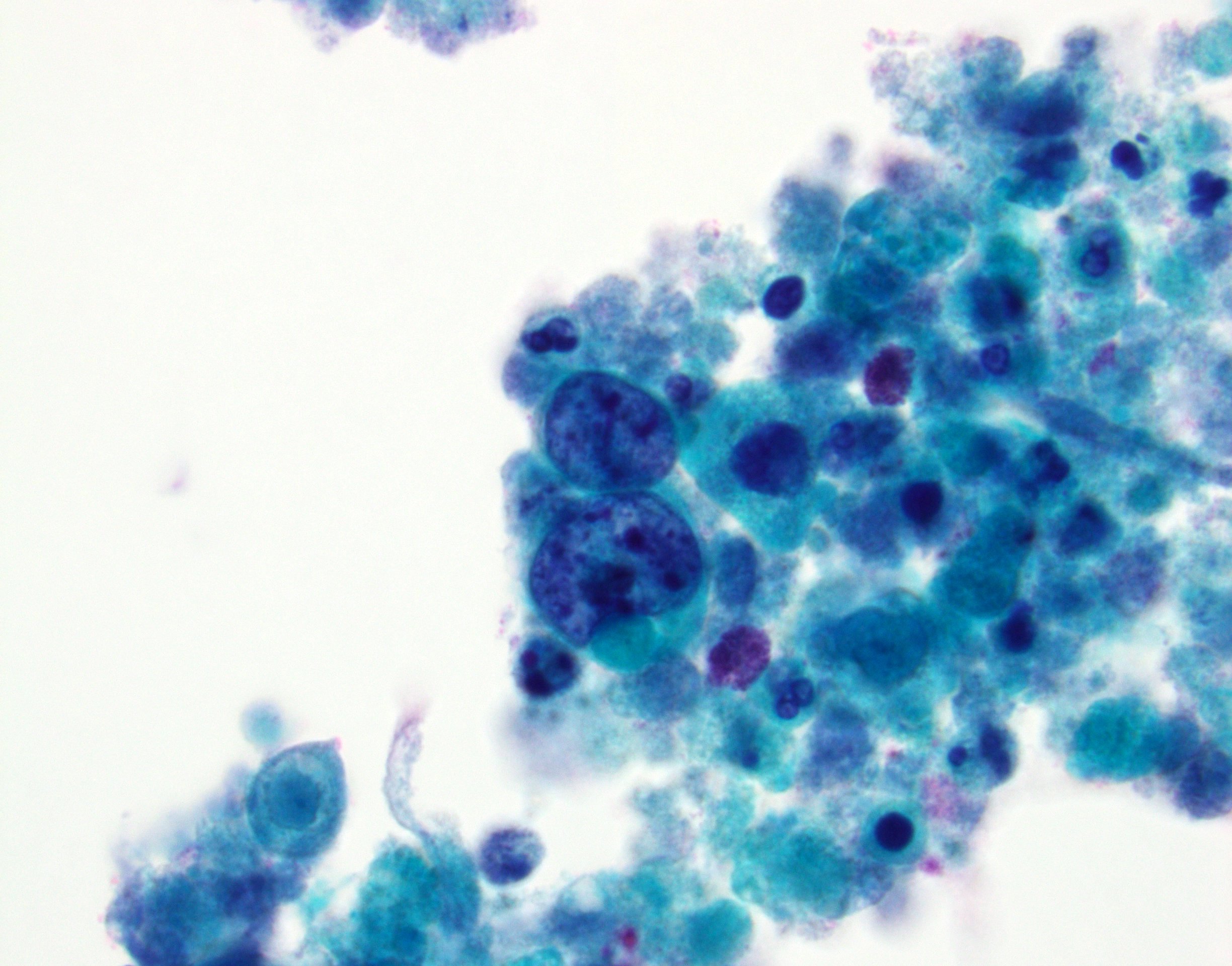
- High grade urothelial carcinoma component: high N:C ratio, nuclear pleomorphism, nuclear membrane irregularity and severe hyperchromasia
- Squamous component: keratinizing cells with high N:C ratio, large and hyperchromatic nuclei, irregular nuclear contour, polygonal cell shape, abundant eosinophilic cytoplasm or dense orangeophilic cytoplasm
- See Paris system for urothelial neoplasia
Cytology images
Contributed by Chunlai Zuo, M.D., M.S.
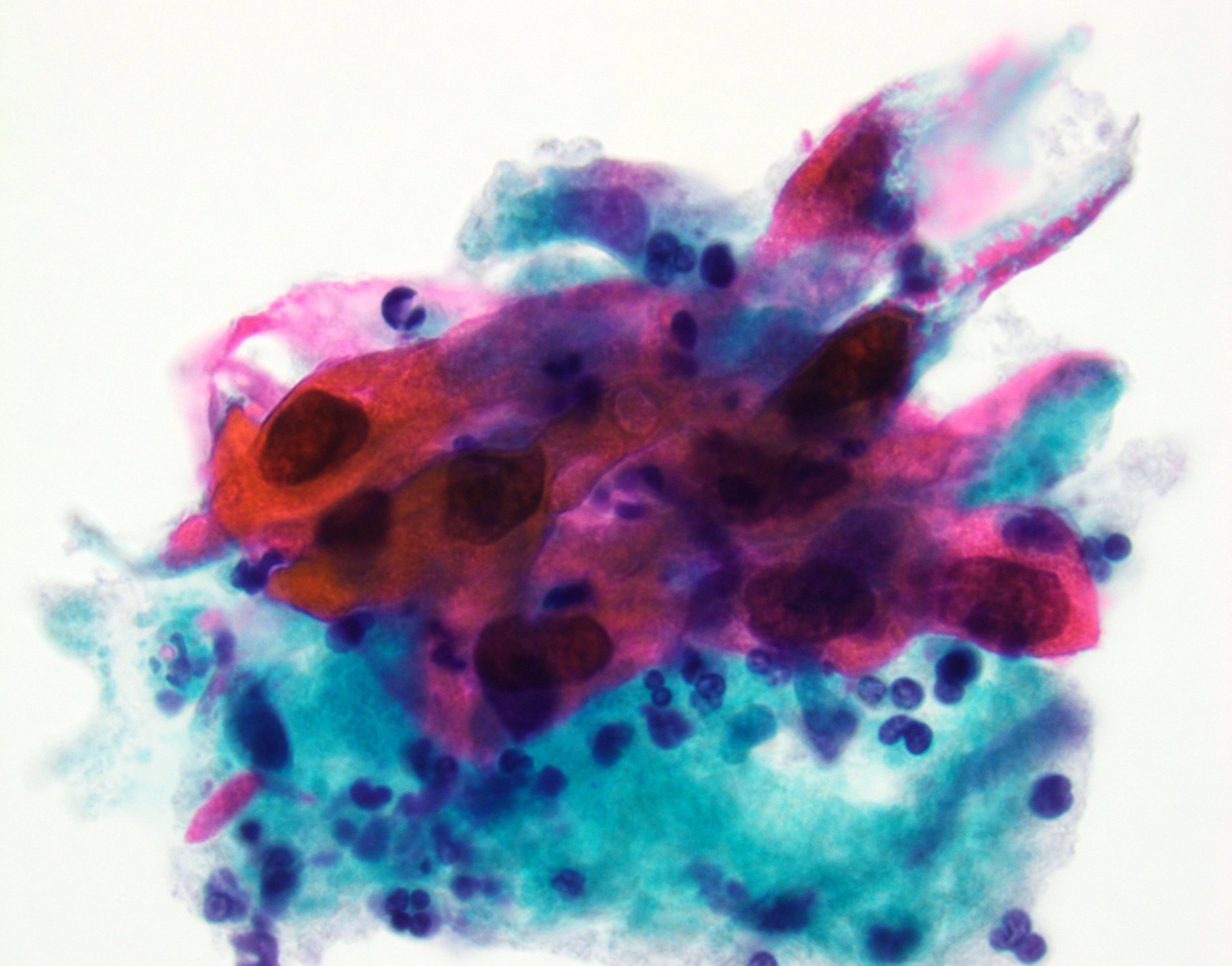
Squamous differentiation
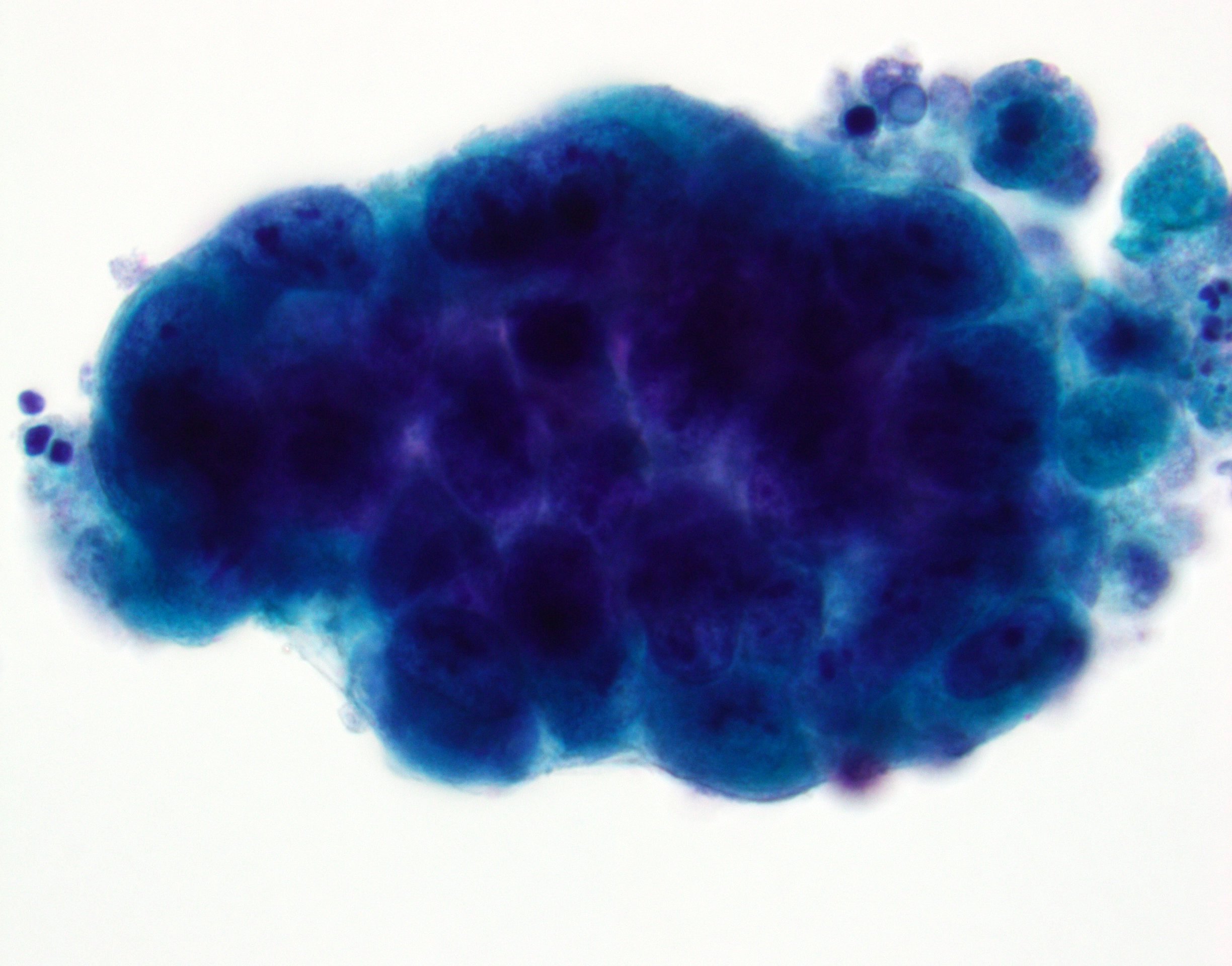
Conventional urothelial carcinoma component
HGUC and necrosis
Images hosted on other servers:

High grade with squamous differentiation
Positive stains
- Squamous component
- CK14, MAC387 (L1 antigen), CK5/6, CK5 / 14, desmoglein, desmocollins (J Clin Pathol 2007;60:332, Virchows Arch 2011;458:301)
- Caveolin-1 (Am J Clin Pathol 2003;120:93)
Negative stains
- Squamous component
- Uroplakins (positive in urothelial component), CK20
Molecular / cytogenetics description
- Basal squamous molecular type by gene expression signature subtyping (Cell 2017;171:540)
- Basal squamous subtype is enriched in TP53 mutations
- Tends to have elevated cell cycle activity and a significant inflammatory signature
Sample pathology report
- Bladder, tumor, transurethral resection:
- Invasive urothelial carcinoma, high grade with squamous (30%) and glandular (10%) differentiation
- Muscularis propria present and involved by carcinoma
- Background urothelial mucosa with squamous metaplasia
Differential diagnosis
- Squamous cell carcinoma:
- Can be associated with Schistosoma haematobium
- Must not have a urothelial carcinoma component
- No criteria to distinguish squamous cell carcinoma with predominately well / moderately differentiated areas and focal poorly differentiated area from urothelial carcinoma with extensive squamous differentiation
- Metastatic squamous cell carcinoma secondarily involving bladder:
- Keratinizing squamous metaplasia with dysplasia or squamous cell carcinoma in situ:
- May be present in adjacent bladder mucosa in cases of bladder primary squamous cell carcinoma
Board review style question #1
Invasive urothelial carcinoma with squamous differentiation is characterized by which of the following?
- High risk HPV in situ hybridization positive
- Intercellular bridges or keratinization
- No clear cut evidence of urothelial component
- p63 positive on immunostain
Board review style answer #1
B. Intercellular bridges or keratinization. The diagnosis is established based on squamous morphology characterized by intercellular bridges or keratinization on H&E stains. Answer A is incorrect because human papillomavirus (HPV) is not commonly associated with urothelial carcinoma with squamous differentiation. In contrast, high risk HPV positivity would support a secondary involvement by cervical, anal or penile squamous cell carcinoma. Answer C is incorrect because, by definition, clear cut evidence of urothelial component must be identified. Answer D is incorrect because p63 is also commonly positive in conventional urothelial carcinoma.
Comment Here
Reference: Urothelial carcinoma with squamous differentiation
Comment Here
Reference: Urothelial carcinoma with squamous differentiation
Board review style question #2
A 50 year old woman presented with hematuria and was found to have a mass involving the bladder posterior wall shown above. Which of the following findings is most supportive of invasive urothelial carcinoma with squamous differentiation over secondary involvement by carcinoma from the other organs?
- Component of uroplakin II positive conventional urothelial carcinoma
- High risk HPV ISH positive
- Mass lesion found at lower uterine segment
- p16 positivity with a diffuse block-like staining pattern
Board review style answer #2
A. Component of uroplakin II positive conventional urothelial carcinoma. Uroplakin II is a highly specific immunohistochemical marker for urothelial differentiation. Answers B, C and D are incorrect since these findings would favor squamous cell carcinoma of cervical or uterine primary over bladder primary.
Comment Here
Reference: Urothelial carcinoma with squamous differentiation
Comment Here
Reference: Urothelial carcinoma with squamous differentiation
